
Case Report | DOI: https://doi.org/10.31579/2578-8868/167
*Corresponding Author: Cindy Díaz, Department of Endovascular Therapy, Universidad Nacional Autonoma de Mexico, Instituto Nacional de Neurologia y Neurocirugia Manuel Velasco (INNN)
Citation: Marco Zenteno, Jorge Balderrama, Alfredo Montenegro, Carmen Vargas, Beatriz Mendez, Miguel Angel Nieto, Cindy Díaz (2021) Endovascular Treatment of intracranial Pial Arteriovenous Fistula in Paediatric Patient. J. Neuroscience and Neurological Surgery. 8(2); DOI:10.31579/2578-8868/167
Copyright: © 2021 Cindy Díaz, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 03 February 2021 | Accepted: 12 March 2021 | Published: 19 March 2021
Keywords: endovascular treatment; pial arteriovenous fistula; paediatric patient
Pial arteriovenous fistula (AVFs) are a rare, although clinically significant, vascular anomaly affecting the pediatric population, consisting of a high-flow connection between one or more pial arteries and the venous. In children, the clinical presentation varies according to age, can present with high output cardiac failure, macrocrania, neurodevelopmental delay, seizures, venous infarctions due to venous stenosis or hemorrhage secondary to venous thrombosis. The treatment, is a multimodal approach, most commonly endovascular, is effective in the obliteration of AVF. A case is presented of a previously healthy infant boy with neurological deficit arising from pAVF of the middle and posterior cerebral artery. The pAVF was successfully treated with endovascular occlusion.
Pediatric pial arteriovenous fistula (pAVF) are rare vascular lesions of the CNS, characterized by direct arterial connections to a pial venous channel, without an intervening nidus. [1] Once thought to be a type of arteriovenous malformation (AVM), they are now recognized as a distinct vascular anomaly. It represent approximately 4% of pediatric cerebral vascular anomalies comprised primarily of arteriovenous malformations (AVMs). The etiology of pAVF is incompletely understood. Theories include the development of dAVF as a sequela of venous sinus thrombosis or secondary to venous sinus hypertension. Presenting symptoms include mass effect, especially if a venous pouch is associated, hemorrhage, seizures, cardiac failure and/or venous hypertension. [2] The high rate of arteriovenous shunting and deep venous drainage decreases the efficacy of microsurgical treatment, and nowadays, endovascular treatment of PAVF is preferable.3Transarterial embolization is the primary method of treatment, although open surgery and radiosurgery have also been employed or a combination. [4]
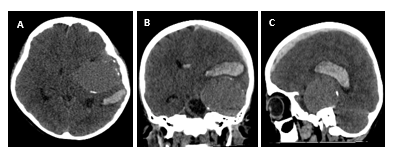
A healthy infant male, suddenly develops headache in thunderclap with altered state of consciousness, presented to an emergency room in coma with anisocoria. Brain CT, revealed acute intraparenchymatous left subdural hematoma, giant vascular dilatation in left temporal lobe (figure 1).
Surgery was performed, with left decompressive craniotomy, acute and intraparenchymatous subdural hematoma was drained, vessels with active bleeding from vascular malformation were identified, 5mm clip was placed, severe brain edema was also observed. An MRI of the brain revealed a giant vascular venous dilatation at left temporal level, with arterio-venous short circuit (figure 2).

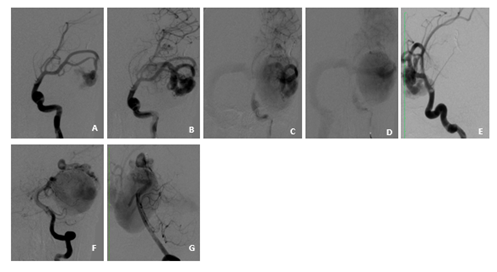
A giant AVF was suspected, and definitive treatment by an endovascular approach was planned. The treatment was performed 90 days after the initial presentation. Diagnostic angiogram demonstrated a multi-hole pial AVF with venous dilation of 54x56 mm which was supplied by enlarged branches of the left posterior cerebral artery (PCA), middle cerebral artery´s medial and posterior basal temporal branches´ lower trunk. Venous outflow drained to a dilated Labbé vein, left lateral sinus and lateral tentorial sinus (figure 3).
Definitive treatment by an endovascular approach was planned.
Embolization were performed with 5 F introducer in the right femoral artery, balanced general anesthesia was used, with non-invasive basic monitoring, anesthetic induction with fentanyl (3 mcg / kg), lidocaine (1 mg / kg) and propofol (3 mg / kg), the anesthetic was maintenance with Sevoflurane 2 V% to maintain 0.8 MAC, the patiente had a stable hemodynamic behavior, due to the high flow characteristics of the fistulae and to avoid the passage of the embolizing material, blood pressure had to be managed dynamically, with intermittent and brief periods of hypotension, administering propofol in bolus 1 mg / kg in 3 times, reaching mean arterial pressures of 62 -64 mmHg, later to corroborate the embolization of the fistulae, blood pressure was increased for a period no longer than 15 minutes, for which epinephrine was administered by intravenous infusion at 0.02 - 0.04 mcg / kg / min until gradually reaching mean arterial pressures of 68 -69 mmHg, suspending the infusion at the end of said period of time.
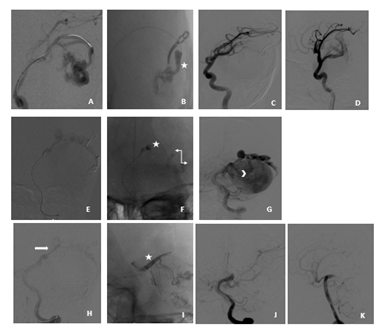
Embolization was undertaken via a 4 F Terumo guide catheter (Terumo Medical Corp, Somerset, New Jersey, USA) and Excelsior SL-10 microcatheter (Stryker Neurovascular). Traxcess 14 guidewire (Microvention) and Mirage™.008” hydrophilic guidewire (Medtronic). With the guiding catheter in the left internal carotid artery, a microcatether was placed on MCA´s the lower trunk and the first embolization was performed. 1 cc of N-butyl cyanoacrylate (NBCA), was safely injected to achieve partial fistulae occlusion (figure 4). Then the guiding catheter is placed in the left vertebral artery, a microcatether was placed in the PCA ipsilaterally and embolization was performed with 1 cc (NBCA) was safely injected to achieve parcial occlusion of the fistulae with passage of embolizing material inside the venous varix, so the microcateter is repositioned (figure 4) in the vein foot and a embolization is performed with 0,8 cc (NBCA) to achieve complete occlusion (figure 4). On the final angiographic control, observed normal anterior circulation was preserved and venous drainage had returned to normal.
The patient was transferred to the pediatric intensive care unit where he recovered for a week without neurological deficit, then hospital was discharge. After a 3 month clinical and MRI control, a complete thrombosis and a reduction of the venous puch was seen. At the time of the last follow-up, the patient was completely asymptomatic without any neurological deficit.
Pial arteriovenous fistula (pAVF) are rare lesional vascular anomalies that pose a high risk of intracranial hemorrhage across all age groups, including children.5 pAVF does not demonstrate a nidus, is supplied from the pial or cortical arteries, and is characterized by abnormal direct high-flow connection between an arterial feeding vessel and draining vein, which has a significant impact on the cerebral blood flow. [6] The reported incidence in literature varies: 3% (13 of 500 AVM) in one to 4.8% (12 of 251 AVM) in another series. [7] Our patient presented with signs and symptoms of a mass effect from a dilated venous pouch and intracerebral hemorrhage.
Embryologically, a fistulae is a likely explanation of abnormally dilated capillary nets that shunt blood from developing arteries to veins. In congenital pial fistulae, the fistulous connection of the dilated capillary nets that develop at this early stage of vascular development randomly persisted with the failure of the structured and more mature capillary network to develop. 8 Most of the arteries feeding the pial AVF open into a single ectatic draining vein frequently associated with large to giant venous varix, and their presence is determined by the high flow across the shunt against venous outflow obstruction. [9] Lasjaunias et al classified between three types of dural arteriovenous shunts that appear in children: (i) dural sinus malformations (congenital malformations of sinus development with giant pouches or malformations of the jugular bulb where thrombosis or occlusion of the sinus outflow is a central clinical concern), (ii) infantile-type dural arteriovenous shunts (high flow, often multifocal lesions with patent sinuses and induced pial arteriovenous shunts) and (iii) adult-type dural arteriovenous shunt. [10]
The treatment of PAVF include multidisciplinary approach, is important to evaluate the location and degree of lesion complexity. [12] The goal of treatment in cortical AVF in young children, even when asymptomatic, is rapid control of the shunt, because of high mortality and worse neurocognitive prognosis when managed conservatively. [10] Increased endovascular experience leading to evolution of techniques and the less invasive nature of the procedure have made endovascular treatment the preferred treatment modality (obliteration rate of 86.5%), offered only to selected superficial fistulae. [13] Endovascular treatment can be done in a few stages to reduce the risk for postoperative hemorrhage by preventing normal perfusion pressure breakthrough in high-flow lesions. [14]
Embolic agents such as NBCA, coils, Onyx 34 have been used for the successful occlusion of the fistulae. Techniques have evolved to counter these such as the use of tandem balloon, balloon-assisted NBCA embolization. [15]
Pial AVF is a rare disease caused by a missed step in vascular development during the early embryonic stage. Treatment, most commonly endovascular, is effective in the obliteration of pAVF in children, with most patients experiencing substantial and durable improvement of clinical symptoms. In our experience, transarterial endovascular embolization using NBCA with or without using coils on the venous side to attain flow control is the treatment of choice with low morbidity. Follow-up is mandatory to look for recanalization and reactive angiogenesis with reopening of the shunt and de-novo dural AVF.
None
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
